A Case of
Chronic Localized Tetanus in an Immunized Patient
(Additional input from the medical community would be appreciated.)
Case Discussion With Video, Pictures & Case Reports (click to jump to video or articles below)
History Of Present Illness / Case Details:
Patient is a 58 year old female physician with past medical history of high cholesterol, celiac disease and multiple food allergies who sustained an open crush fracture of the left big toe in June 2022 after a heavy double glass and metal shower door fell on her toe. She was seen in the ER and received wound care with tetanus booster and trephination of toenail. 2-3 days after injury intermittent twitching was noted in the small muscles surrounding the injured toe. One week after injury, twitching worsened around the medial left foot, progressed to the lateral toes of the left foot, then gradually progressed further up the left leg. Once twitching reached the gluteal muscles (ascending spread), it spread to the all extremities and back. There were several strong tonic contractions of gluteal muscles which lifted the patient off of the couch involuntarily. At this time patient had concern for tetanus and sought initial ID consult. Labs done included Creatinine Kinase which was 602 with normal CBC, CMP and negative blood cultures.
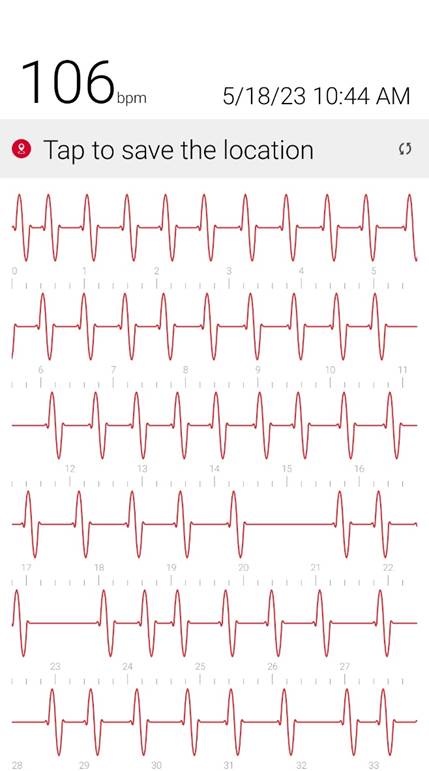
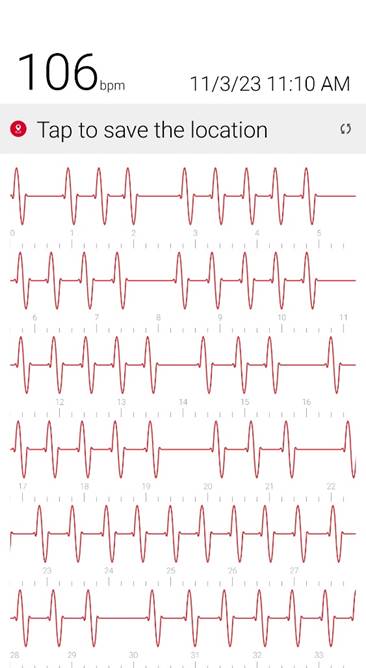
Initial ID consult diagnosed local tetanus based on clinical symptoms and recommended oral Metronidazole 500mg every 6 hours as an outpatient. Autonomic involvement developed with tachycardia and cardiac arrhythmia, along with episodes of sudden sweating. Loud noises made twitching/spasms worsen. Intermittent twitching continued to be present bilaterally in the body, face, jaw & tongue. Symptoms were suppressible with benzodiazepine. Tetanus IM IG 500 IU was recommended and obtained. After initial 2 week course of metronidazole was discontinued symptoms worsened again when patient would walk. Multiple trials of oral Metronidazole 500mg every 6 hours were attempted with some improvement while on the antibiotic but then return and worsening of symptoms again once antibiotic was discontinued.
Patient was hospitalized in August 2022 for IV (Intravenous) metronidazole which helped reduce (but not eliminate) symptoms for about one month. MRI of the left toe showed still healing fracture and ortho consult did not recommend surgical intervention at that time. Multiple neurology consults were obtained to rule out neurological cause of symptoms given the unusual presentation and all neurology consults felt this was not primarily a neurological issue and she was referred back to Infectious Disease for management. EMG & MRI of the brain were done and were both normal. (Patient was advised to continue benzodiazepine during initial EMG so any possible exaggerated F-response and spasms were suppressed by benzodiazepines during the EMG). During all physical exams involuntary muscle spasms/ twitching of the left foot/toes were noted involving both agonist and antagonist muscles.
A second Tetanus Vaccine (Tdap) was recommended 4 weeks after the initial tetanus booster she received in the ER (patient also had had a full set of childhood tetanus vaccines). Three days after receiving the second tetanus vaccine since injury, patient developed new onset full body pins & needles which days later developed into a sensory peripheral neuropathy in her bilateral feet & left hand. Neurology felt this was likely a vaccine side effect due to excess tetanus vaccine/antibodies as there was partial response of the new onset sensory neuropathy to IVIG treatments which were started to treat the post vaccine sensory neuropathy. Neurology felt that the neuropathy was not secondary to metronidazole since it responds partially to monthly IVIG.
Tetanus antibody levels consistently show patient is fully hyperimmunized (>7.0 IU/ml). Tetanus antibody levels did not decrease significantly with time over 26 months, even though diphtheria antibody levels (given in the same Tdap vaccine) steadily declined with time as expected. (Suggesting continued immune exposure to tetanus toxin)
A trial of Hyperbaric oxygen was recommended to aid in fracture healing (with the thought that clostridium tetani would not remain active once fracture was fully healed) Hyperbaric oxygen helped reduce local twitching in the left foot and reduced generalizations and autonomic involvement which would occur with walking or increased pressure on the left great toe. (In the literature Tetanus toxins (tetanospasmin and tetanolysin) have been noted to be oxygen labile.) Hyperbaric oxygen was discontinued after patient developed cataracts as a side effect.
Local muscle twitching around the left toe/foot worsened off hyperbaric oxygen. Symptoms always began with hyperesthesia in the left big toe, muscle twitching around the left toes and foot, twitching progressed up the left leg
incrementally, then once twitching had reached the spinal level, muscle twitching spread to the bilateral muscles of the body with cardiac arrhythmia & autonomic involvement/ sweating. A trial of antibiotic Keflex (cephalexin ) was suggested, which only at high dose (1000mg PO every 6 hours), helped keep spasms localized to the left foot mostly but symptoms would worsen and generalize if antibiotic Keflex (cephalexin) was stopped for more than 2 days. Benzodiazepine was increased to every q6 hours to reduce muscle twitching that had become constant in the left foot. Symptoms improve when patient does not walk or avoids any pressure or bending of left big toe and symptoms worsen when patient walks or stops antibiotic and has been unable to stop antibiotic for the past year and a half without worsening of symptoms. When antibiotic is stopped for 2 days bilateral jaws begin to snap shut intermittently involuntarily and cardiac arrhythmia/ heart block reoccurs. Symptoms worsen further after 4 days off antibiotic. Local
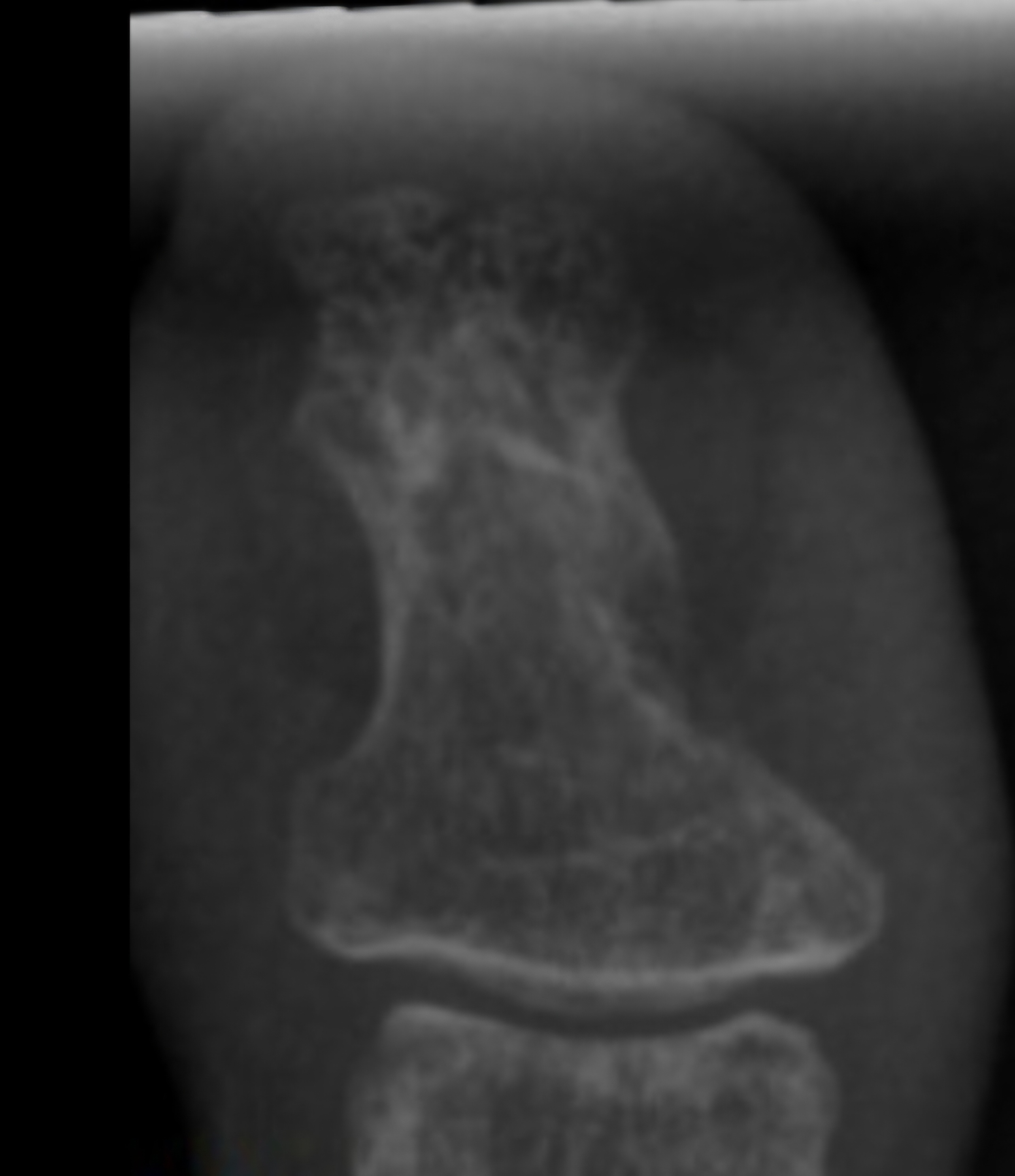
MRI one year after injury showed some abnormal signal. (Clostridium tetani infection generally has no clear radiological findings or lab confirmatory tests and is generally a clinical diagnosis). Patient sought consults with multiple infectious disease doctors in New York but despite repeated worsening off antibiotics, clear clinical signs of local tetanus in the left foot, progression of spasms / twitching up the left leg with generalization and autonomic symptoms including heart block and involuntary jaw closure within days of stopping antibiotics or walking more than small amounts, infectious disease physicians in New York (who have not had experience with tetanus) have been conflicted on the diagnosis and of little help. (The medical literature reports that the presentation of tetanus in an immunized patient would typically be different than the presentation in an unimmunized patient and instead of presenting with full body tetany, an immunized patient would present with an ascending pattern of spasms / twitching up the affected limb from the localized point of infection with progression to generalization as in this case.)
Patient sought surgical consult with a bone specialist surgeon who diagnosed patient clinically with tetanus osteomyelitis & surgical debridement of the left big toe (distal bone) was attempted 2 times. First surgery involved bone debridement of the medial side of the toe with placement of antibiotic laden calcium stimulan beads. The first surgery did not resolve the symptoms and actually worsened tetanus symptoms for about a month post surgery. One episode of brief full left leg tetany occurred in the first month post surgery . During the surgery, the surgeon visually graded the bone as "infected" with an infection level of 4 out of 4, stating the bone appeared much softer than it should be. (The surgeon specializes in bone surgery and stated he had never seen bone that looked like this) Cultures (anaerobic, aerobic and fungal) were negative but the surgeon and literature advises that anaerobic cultures rarely come back positive (accuracy is only about 30% in confirmed positive cases).
A second bone debridement surgery was attempted on the lateral side of the left big toe. Metronidazole was discussed as being a possible ideal antibiotic for the antibiotic laden calcium stimulan beads to be inserted during the surgery but surgeon advised the pharmacy was unable to obtain the appropriate dilution of metronidazole so vancomycin was used in the antibiotic laden calcium beads instead. (vancomycin has no known efficacy against clostridium tetani). Each surgery temporarily worsened twitching/spasms for one month post surgery requiring increased doses of antibiotic (Metronidazole 500 twice daily was added to Keflex (cephalexin) 1000mg 4 times daily for several days post surgery due to worsening spasms, and spasm suppressing benzodiazepine was increased to control symptoms.
Plan during the first surgery was to submit lab samples for 21s rRNA PCR testing for clostridium tetani however the bone sample from first surgery was placed in the incorrect media so PCR testing of the clearly infected sample could not be performed at all. Surgical sample from the second debridement surgery (taken from a different site on the toe) was noted to be visually "clean" during the surgery (without signs of infection). It was sent to Mayo Clinic for PCR testing and results were negative however infectious disease consult at Columbia Hospital states that Mayo clinic PCR results are often inaccurate in their opinion and they recommend if more samples are to be sent they should be sent to the University of Washington as they find their testing to be more accurate. Local Tetanus symptoms and generalization when antibiotics were stopped continued to occur after the second surgery.
One infectious disease physician suggested high dose Bicillin-LA Intramuscular injections (Benzathine Penicillin G). 2.4 Million units three times a week for 2 weeks did improve symptoms. Oral Keflex (cephalexin) was able to be temporarily discontinued (benzodiazepine was continued) and patient was able to walk more without exacerbation or generalization however approximately one week after 2 week course of Bicillin-LA was discontinued, spasms and generalization returned.
Oral Keflex (cephalexin) 1000mg 4 times a day & IM Bicillin LA 2.4 million units 3 times a week were restarted with improvement in bilateral body muscle twitching but twitching / spasms locally in the left toes and foot continued. This regimen was continued for 7 weeks. One day after discontinuing oral Keflex (cephalexin) (and 3 days after the last bicillin IM shot) spasms again began at the left big toe, left toes and left foot, progressed up the left leg to the left gluteal muscles and again once the spinal level was reached spasms spread to the right side of the body and then upper body and by 1 and 1/2 days after all antibiotic was discontinued, arrhythmia/heart block began again. Oral Keflex 1000mg 4 times a day was restarted (cephalexin). Benzodiazepines had been continued throughout.
Multiple attempts (>12) have been made to stop antibiotics, and consistently each time antibiotics are stopped the symptoms return. No cardiac abnormalities or symptoms of generalization are seen while patient remains on antibiotic. This presentation appears consistent with multiple case & data below which has demonstrated that in an immunized patient, tetanus toxin takes a retrograde neuronal route before reaching the CNS and generalizing since the blood bourne route is blocked by antibodies if immunized.
Surgeon has recommended allowing more time for bone healing while remaining on antibiotics and spasm/ twitch suppressant benzodiazepines (current regimen is oral Keflex (cephalexin) 1000mg 4 times a day with alprazolam 1mg q 4-6 hours which keep the symptoms localized to the left toes and left foot and minimal at that dose of alprazolam. During exacerbations from walking when generalizations start, oral metronidazole 500mg twice a day is added for several days when needed which stops the generalization although antibiotic appears to be becoming somewhat less effective. Attempting a needle biopsy was discussed to confirm the diagnosis with another attempt at PCR testing prior to considering amputation however there is concern that the biopsy needle may spread the bacteria further than the distal metatarsal bone of the left big toe where it is believed to be contained which was the site of the initial crush fracture. Surgeon is also concerned that amputation could spread the bacteria further in the foot during the surgery. Avoiding amputation would be preferred if possible.
Additional input from the medical community with experience with tetanus would be appreciated to both confirm the diagnosis and suggest treatment to resolve this case. Email to bookappt@outlook.com
|
Summary of treatments tried thus far: |
Effect: |
|
tetanus booster vaccine in ER on the day of the toe crush fracture with brief initial Course of Augmentin (7 days?) |
Not effective |
|
Intermuscular Tetanus IG |
Not effective |
|
2nd tetanus booster vaccine |
Not effective Caused side effect of bilateral Peripheral Sensory Neuropathy believed to be from excess tetanus antibody |
|
multiple courses of oral metronidazole 500mg every 6 hours (4-6 courses) with alprazolam 0.5mg every 6 hours as needed added for spasms |
-worked while on antibiotics, tetanus symptoms return after antibiotic is stopped. |
|
hospitalization with IV metronidazole 500mg every 6 hours for 2 weeks |
-worked while on antibiotics, tetanus symptoms return after antibiotic is stopped. |
|
approximately 6 months of hyperbaric oxygen treatments |
Kept spasms local to foot and prevented generalization without antibiotics but only worked for 6 months and had to be stopped due to side effect of cataract development. |
|
Keflex (cephalexin )500mg orally every 6 hours |
Not effective |
|
Keflex (cephalexin )1000mg orally every 6 hours with alprazolam 0.5mg q4-6 hours as needed for spasms |
- helpful to keep symptoms mostly local to the left foot/toes unless walking more than approximately 10 minutes, but with constant foot /toe spasms occurring regularly but without generalization. |
|
2 debridement surgeries with antibiotic laden beads (one with a cephalosporin in the beads and one with vancomycin in the beads) |
Initially surgery worsened tetanus spasms and caused generalization for one month, reduced by increasing antibiotic but had no overall improvement after surgery. |
|
trial of high dose injectable penicillin (Bicillin LA) 2.4 million units 3 times a week for 3 months (meant to be similar to 3 months of intravenous (IV) penicillin) |
– not effective. |
|
Current regimen is: Keflex 1000mg orally every 6 hours with alprazolam 1mg orally every 4-6 hours for twitching/spasms with occasional addition of low dose metronidazole (500mg PO BID for 2 to 3 days) when symptoms worsen if walking more. (*note: – full course of metronidazole 500mg every 6 hours orally alone at this point 2.5 years after injury becomes ineffective after about 4 days so some resistance to metronidazole alone is suspected at this point. Currently if patient misses even several doses of antibiotic (for example 1 dose 2 days in a row) twitching will worsen around the left foot/toes |
– effective at keeping symptoms local to the feet/ toes with much reduced spasms in the foot/toes unless walking for more than about 10-15 minutes, tetanus still generalizes via ascending spread if antibiotics are stopped. (spasms/twitching will ascend the left leg and spread to the right side of the body and face/jaw with heart block if antibiotics are stopped.) |
1) Videos of Left Toe & Foot Spasms/Twitching:

2) Video Of Mild Jaw Spasms Seen At Rest After Stopping Antibiotic For Only 2 Days
(Spasm Of Jaw Becomes More Severe And Frequent After 4 Days Off Antibiotic):

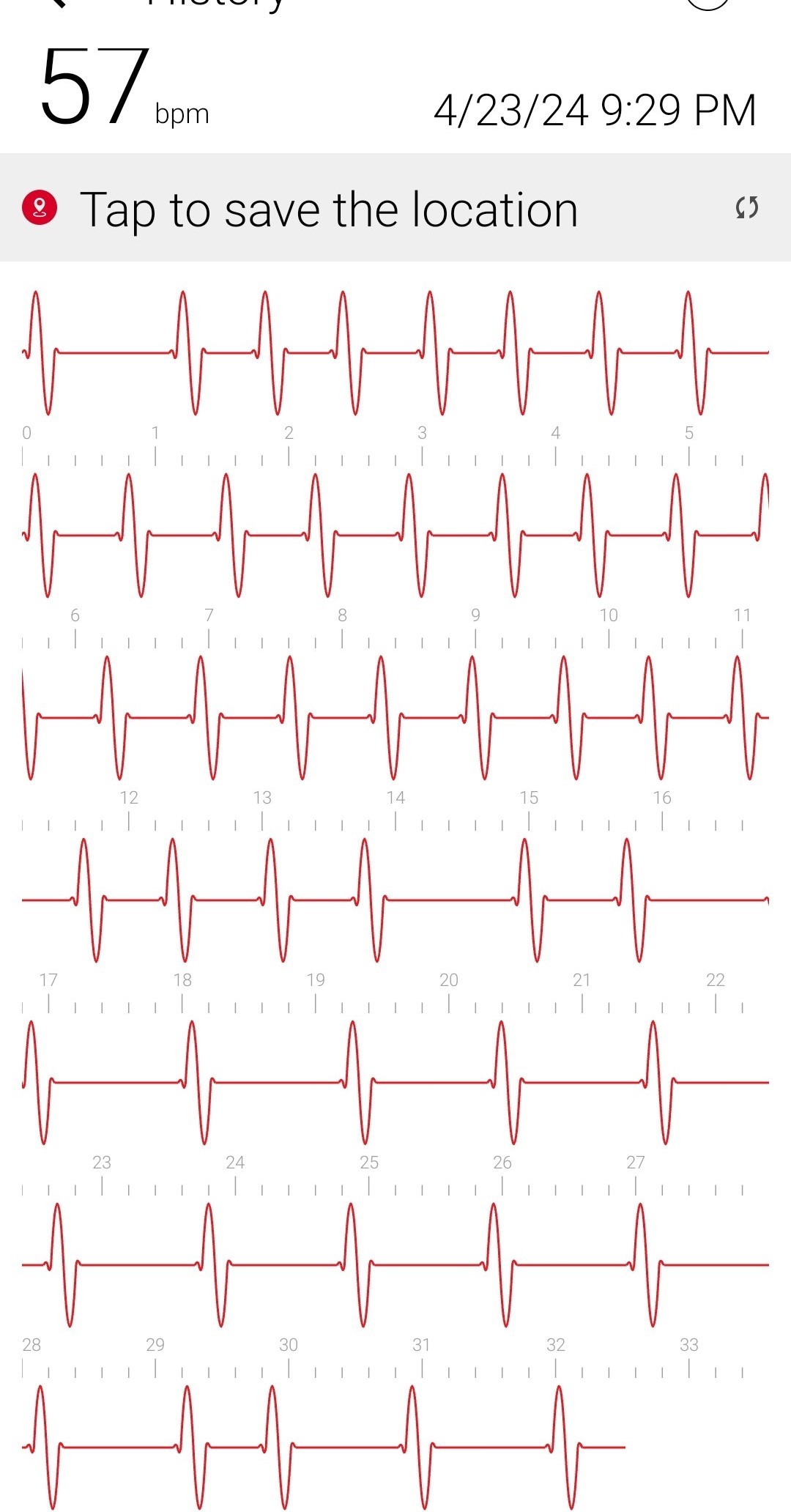
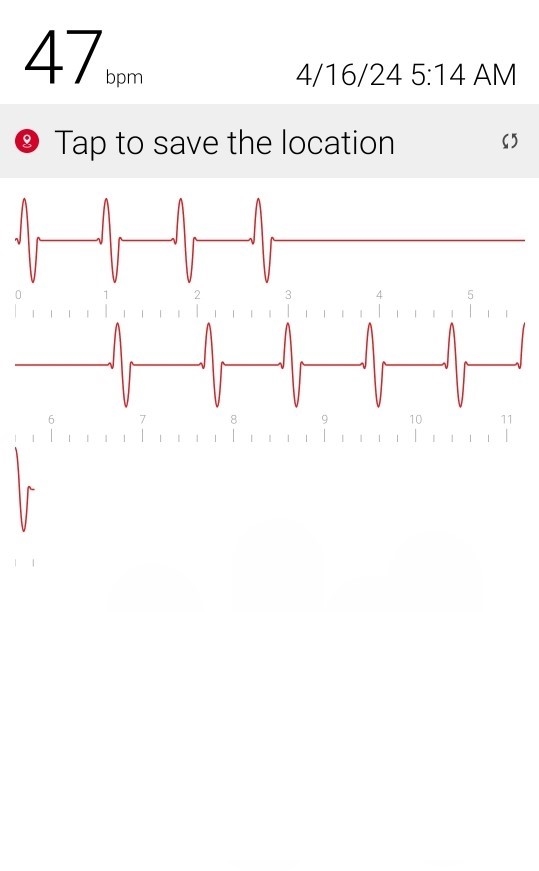
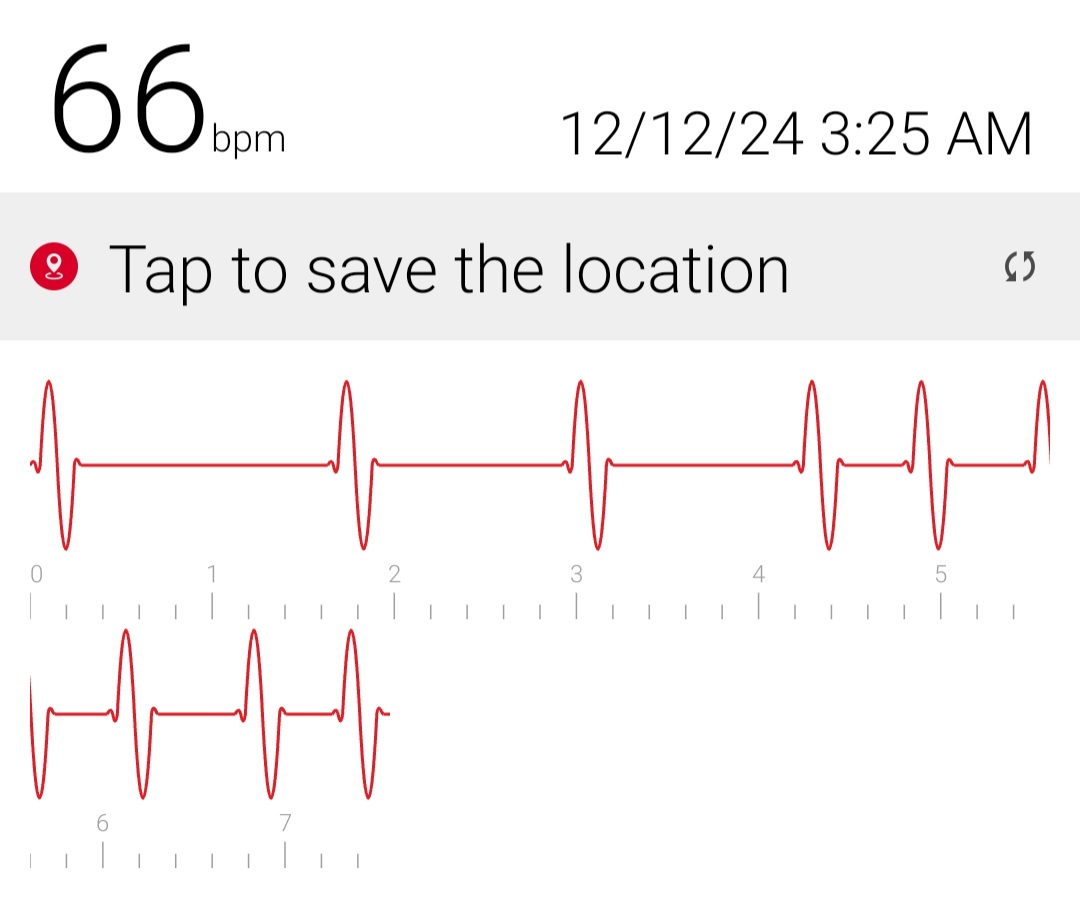
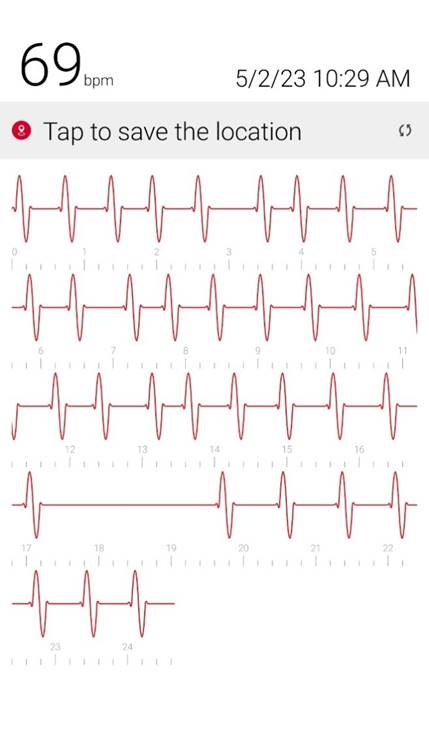
3) Cardiac Arrhythmia / Heart Block occurs during generalizations
When antibiotic is discontinued or with increased walking, rhythm returns to normal when antibiotic is restarted after a few days.

4) Video Of Various Small Fiber Twitches Seen When Generalization Begins:
Photos
Left Great Toe 6 weeks post second bone (lateral) debridement surgery & left / right Great Toe comparisons:



Left Great Toe 12 weeks post first bone debridement surgery & left / right Great Toe comparisons:




post first bone debridement surgery (medial side)
Relevant Articles, Case Reports, and Experimental Data:
(On the mechanism of local tetanus and generalization in immunized patients as well as case reports of chronic tetanus)
(most relevant portions of each report have been highlighted in yellow/ orange)
1. Relapsing tetanus (a case report). J Postgrad Med 1981;27:184. Bhatt A D, Dastur FD https://journals.lww.com/jopm/citation/1981/27030/relapsing_tetanus__a_case_report__.11.asp
Full Article:

"However, if the toxin in the blood is neutralised by anti-toxin, the toxin can only ascend to the brain or spinal cord by the local neural pathway. There, it abolishes central inhibition. This leads to local muscle stiffness which slowly ascends to other parts of the body as the toxin spreads upwards in the spinal cord. This is local tetanus which leads to tetanus ascendans."
"localised, deep wound on the sole of the right foot might have renewed toxin production when the patient started to walk on the 40th day. The pressure exerted on the sole of the foot could have forced the spores deeper into an avascular area and provided the anaerobic conditions necessary for germination. In the presence of circulating antitoxin, the toxin could take only the pathway of regional motor nerves. This contention is supported by the sequence of tetanus in the second episode. It started in the right foot spreading up the right lower limb, right side of the abdomen, then spreading to involve the opposite side and finally ascending to involve the rest of the body."
2. An Unusual Case of Evolving Localized Tetanus Despite Prior Immunization and Protective Antibody Titer
Biswaraj Tharu, 1 Safa Ibrahim,2 Munir Shah,3 Sijan Basnet,4 and Terrence Park1 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7466034/
"Only two case reports of localized tetanus in previously immunized patients have been reported so far, making this the third one. Also, this is the first case of its kind to demonstrate evolving localized tetanus." "Upon further review, the patient recalled cutting himself on the right middle finger with a nail while removing the carpet a week ago. This was followed by pain and stiffness in the right hand, but the patient did not seek medical care as it did not bother him. The patient and his mother reported completing all five childhood vaccinations". "No obvious injury was noted on his affected hand where he indicated he had a puncture wound. He had a carpopedal spasm of his right hand." "Localized tetanus is uncommon and usually presents as persistent muscle contractions in the affected traumatic area." " This is the first case of its kind to report evolving localized tetanus. The diagnosis of tetanus is entirely clinical." "it is very important to note that the possibility of tetanus infection with protective levels of antibodies cannot be excluded"
3. Present Data on the Pathogenesis of Tetanus by GN KryzhanovskyID: 769068 DOI: 10.1007/978-3-0348-7090-0_34 https://link.springer.com/chapter/10.1007/978-3-0348-7090-0_34
Full Article:
"The clinical picture of disease greatly depends on which neuronal pathways are involved in the process of toxin transport into the CNS. At the entrance of toxin only by the regional neural pathway there arises a local and ascendens tetanus in animals and partial tetanus in human. This situation occurs if the spread of toxin with blood is blocked by antitoxin."
4. On The Pathogenesis Of Ascending And Descending Tetanus G. N. Kryzhanovskiy, L. A. Pevnitskii, V. N. Grafova, and A. A. Polgar
Full Article:

“local tetanus in human beings are encountered more and more frequently. As a rule, local tetanus is observed in patients who have been actively or passively immunized i.e., in those cases where dissemination of the toxin by the blood was excluded or essentially limited.”
"After blocking the circulatory route of the toxin spre.ad by means of tetanus antiserum, tetanus develops according to the ascending type" "Ascending tetanus is based upon toxin spread from the site of administration along the regional nerve"
5. Pathogenesis of local tetanus in rats: neural ascent of tetanus toxin L E King Jr, A A Fedinec PMID: 4275259 DOI: 10.1007/BF00499434
https://link.springer.com/article/10.1007/BF00499434
"The mechanisms of local tetanus or unilateral tetanus toxin induced paralysis due to intramuscular injections were studied in adult Wistar rats" "Tetanus toxin was detected in rat sciatic nerve trunks and blood in the following sequence: injection site; ipsilateral epineurium; blood and ipsilateral perineurium; contralateral epineurium. The blood and the nerve segment closest to the injection site contained toxin for at least 24 h " "Toxin was detectable in the contralateral nerve trunk (epineurium) only after being detected in the blood. " local tetanus appears to be due to peripheral nerve toxin transport in the perineurial tissue spaces to the spinal cord."
6. A Toe That Pointed The Wrong Way: An Unusual Presentation Of Tetanus Krishnarpan Chatterjee, Anirban Ghosh, and Rimi Som Sengupta " https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4750318/
"Localized tetanus is a rare variant affecting muscles near the site of inoculation. It is usually mild but may progress to generalized tetanus. "
7. An Unusual Case Of Chronic Relapsing Tetanus Associated With Mandibular Osteomyelitis Yasuhito Wakasaya 1, Mitsunori Watanabe, Masahiko Tomiyama, Chieko Suzuki, Mandy Jackson, Masahiro Fujimuro, Tamaki Kimura, Yusuke Seino, Takeshi Kawarabayashi, Yukiko Yamamoto-Watanabe, Etsuro Matsubara, Ikumi Shirahama, Ayumi Takamura, Naoko Nakahata, Mikio Shoji https://pubmed.ncbi.nlm.nih.gov/19652437/
"in spite of injections of tetanus toxoid, symptoms of tetanus returned when the administration of metronidazole was discontinued "
8. Localized tetanus in a child - L Fiorillo 1, J L Robinson Ann Emerg Med . 1999 Apr;33(4):460-3. doi: 10.1016/s0196-0644(99)70314-8.
https://pubmed.ncbi.nlm.nih.gov/10092728/
"We present the case of a child who had localized tetanus despite previous partial immunization."
9. Elevated antitoxin titers in a man with generalized tetanus - T Pryor 1, C Onarecker, T Coniglione Affiliations expand PMID: 9071251 J Fam Pract . 1997 Mar;44(3):299-303 https://pubmed.ncbi.nlm.nih.gov/9071251/
"This report describes severe, generalized tetanus in a 29-year-old man who had received a primary series as a child and two booster injections. Serum obtained before administration of tetanus immune globulin showed antibody titers to tetanus greater than 100 times the level considered protective. "
10. Chronic tetanus: Clinical report and histochemistry of muscle : Dr. Winthrop S. Risk MD, PhD, Dr. E. Peter Bosch MD, Dr. Jun Kimura MD, Dr. Pasquale A. Cancilla MD, Dr. Kenneth H. Fischbeck MD, Dr. Robert B. Layzer MD First published: September/October 1981 https://doi.org/10.1002/mus.880040502 https://onlinelibrary.wiley.com/doi/10.1002/mus.880040502
A patient who was partially immune to tetanus developed nonfulminant tetanus after a minor injury. Manifestations of the disease persisted for over 17 months." "This observation supports the existence of chronic tetanus and provides morphologic evidence for a peripheral action of tetanus toxin in humans."
11. A case of tetanus infection in an adult with a protective tetanus antibody level Kristan E Vollman 1, Nicole M Acquisto 2, Ryan P Bodkin 3 Affiliations expand PMID: 24211286 DOI: 10.1016/j.ajem.2013.10.025Am J Emerg Med . 2014 Apr;32(4):392.e3-4. doi: 10.1016/j.ajem.2013.10.025. Epub 2013 Oct 15. https://pubmed.ncbi.nlm.nih.gov/24211286/
"We report the case of a 31-year-old male that presented to the emergency department (ED) with a 2-day history of neck and jaw pain. He reports puncturing his hand with a rusty nail 10 days prior." "Despite his presentation of tetanus infection and rule out of other causes for his symptoms, his tetanus antibody level was reported at 8.4 U/mL, which is considered to be protective. A tetanus antibody level that is adequate for protective immunity should not preclude a patient from treatment of tetanus infection."
12. A systematic review of tetanus in individuals with previous tetanus toxoid immunization JP Hopkins,1, 2,* C Riddle,3 M Hollidge,3 and SE Wilson4, 5 Can Commun Dis Rep. 2014 Oct 16; 40(17): 355–364. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5864474
"51 unique articles published from 1946-2013 were included in the review. The articles described 359 cases of clinical tetanus in individuals with prior receipt of one or more doses of tetanus toxoid vaccine and/or levels of tetanus antibody titres generally considered protective. " "this report clearly documents that tetanus cases can occur in individuals previously immunized with tetanus toxoid vaccine. Clinicians should not rule out tetanus when clinical symptoms suggest it, regardless of the vaccination history." "Tetanus spores are ubiquitous and this report clearly documents that tetanus cases can occur in individuals previously immunized with tetanus toxoid vaccine. Clinicians should not rule out tetanus when clinical symptoms suggest it, regardless of the vaccination history. "
13. An unexpected tetanus case Onder Ergonul 1, Demet Egeli 2, Bulent Kahyaoglu 3, Mois Bahar 2, Mill Etienne 4, Thomas Bleck 5 Lancet Infect Dis . 2016 Jun;16(6):746-752. doi: 10.1016/S1473-3099(16)00075-X. https://pubmed.ncbi.nlm.nih.gov/27301930/
"unexpected cases can occur in individuals who have been previously vaccinated. We report a case of generalised tetanus in a 22-year-old woman that arose despite the protective antitoxin antibody in her serum." "Tetanus can present with unusual clinical forms; therefore, the diagnosis and management of this rare but difficult disease should be updated."
14. Tetanus and tetanus neurotoxin: From peripheral uptake to central nervous tissue targets Aram Megighian, Marco Pirazzini, Federico Fabris, Ornella Rossetto, Cesare Montecucco First published: 24 February 2021 https://doi.org/10.1111/jnc.15330
"TeNT enters the general circulation, binds to peripheral motor neurons and sensory neurons, and is transported retroaxonally to the spinal cord. It then enters inhibitory interneurons and blocks the release of glycine or GABA causing a spastic paralysis."
15. Uncommon Progressive Systemic Tetanus: A Case Report Monitoring Editor: Alexander Muacevic and John R Adler Reinaldo Sanchez-Grillo,1 Esteban Zavaleta-Monestel,corresponding author2 Eduardo Ruiz-Munguia,3 José Pablo Díaz-Madriz,2 and Carolina Rojas-Chinchilla4 Cureus. 2023 May; 15(5): e38383. Published online 2023 May 1. doi: 10.7759/cureus.38383 PMCID: PMC10231406 PMID: 37265915 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10231406/
"This case highlights the importance of considering tetanus in the differential diagnosis even if the vaccination schedule is complete, especially if there are spasms, convulsions, or a history of wounds or bites. "
16. Tetanus Overlooked Due to the Involvement of Multiple Departments: A Case Report Monitoring Editor: Alexander Muacevic and John R Adler Takanori Ohno,corresponding author1 Masashi Kanazawa,1 Takaaki Nakano,1 Masaaki Takemoto,1 and Toshitaka Ito1, Cureus. 2023 Oct; 15(10): e48066. Published online 2023 Oct 31. doi: 10.7759/cureus.48066 PMCID: PMC10689120 PMID: 38046504 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10689120/
"she visited our hospital and was suspected of having tetanus after consulting with nine different departments over seven days from the initial visit. In developed countries, tetanus prevalence has declined due to immunization, leading to clinicians' lack of experience in diagnosing it."
Articles on Clostridium Tetani Susceptibility & possible treatment options:
Benzathine penicillin, metronidazole and benzyl penicillin in the treatment of tetanus: a randomized, controlled trial A V Ganesh Kumar 1, V M Kothari, A Krishnan, D R Karnad Ann Trop Med Parasitol . 2004 Jan;98(1):59-63. doi: 10.1179/000349804225003037 https://pubmed.ncbi.nlm.nih.gov/15000732/
"Although the three antibiotic regimens investigated appear equally effective, benzathine penicillin offers the convenience of a single, intramuscular injection instead of the 10 days of therapy needed with the other two drugs"
Isolation and Antibiogram of Clostridium tetani from Clinically Diagnosed Tetanus Patients Hajra Hanif 1, Awais Anjum 2, Naeem Ali 1, Asif Jamal 1, Muhammad Imran 1, Bashir Ahmad 1, Muhammad Ishtiaq Ali 1 Am J Trop Med Hyg . 2015 Oct;93(4):752-6. doi: 10.4269/ajtmh.15-0040. Epub 2015 Jul 14. https://pubmed.ncbi.nlm.nih.gov/26175031/
In "80 clinically diagnosed tetanus patients" "C. tetani isolatesshowed susceptibility to cefoperazone, chloramphenicol, metronidazole, penicillin G, and tetracycline,but were found to be resistant to erythromycin and ofloxacin"
Localized tetanus in immunized mice Neurotoxicology . 2009 Jul;30(4):697-701. doi: 10.1016/j.neuro.2009.05.004. Epub 2009 May 22. Localized tetanus in immunized mice Paul S Fishman 1, Deborah A Parks, Thomas Bowen, Christopher C Matthews https://pubmed.ncbi.nlm.nih.gov/19465055/
"Although vaccination dramatically increases resistance to tetanus toxin, by virtue of its extremely high potency, the toxin can produce prolonged localized tetanus even in vaccinated animals with relatively small amounts of protein. "
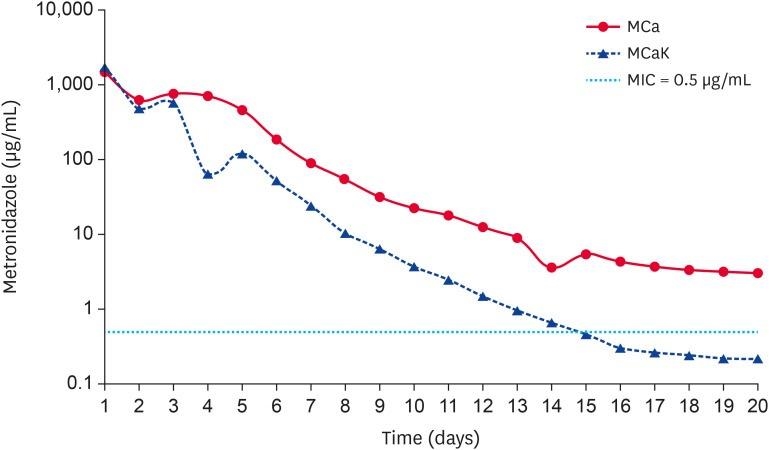
Elution profiles of metronidazole from calcium sulfate beads Burasarin Ithisariyanont, Saranya Poapolathep, Amnart Poapolathep, Pareeya Udomkusonsr J Vet Sci.
2023 Nov; 24(6): e74. Published online 2023 Sep 18.doi: 10.4142/jvs.23166 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10694377/
(This experimental data highlights that higher doses of metroniazaole (ex: 500mg) in calcium sulfate beads may be a surgical option with debridment in keeping MIC above dosages needed to kill C Tetani for greater days at higher dosages in theory.)
_________________________________________________________________________________________________
Further articles & Case Reports on recurrent, local, or atypical tetanus or tetanus in fully immunized patients:
Atypical tetanus--towards an understanding. Dastur, FD; Shahani, MT Journal of Postgraduate Medicine 29(2):p 59-61, Apr–Jun 1983.
https://pubmed.ncbi.nlm.nih.gov/6313914/
"found adjacent to the precipitating lesion" "affected muscles... are first transformed into a state of overactivity"
Dastur, F. D. and D'Sa, J.: Tetanus-Present Knowledge and Experience, In, "Progress in Clinical Medicine in India." Editor: M. M. S. Ahuia, Third Series, Arnold-Heinemann, New Delhi, 1979, p. 71.
Recent advances in tetanus. Dastur FD, Nair KG.J Assoc Physicians India. 1979 Jun;27(6):551-7.PMID: 528515
Tetanolysin Tetanolysin causes local tissue damage that enhances spore germination by creating a locally anaerobic environment. From: Nonhuman Primates in Biomedical Research (Second Edition), Volume 1, 2012 https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/tetanolysin
The mouse toxicity bioassay as a laboratory confirmation test for tetanus L Delbrassinne, J Vanderpas, Acta Clin Belg . 2015 Feb;70(1):77-8. doi: 10.1179/2295333714Y.0000000074. Epub 2014 Sep 16.
https://pubmed.ncbi.nlm.nih.gov/25224543/
A systematic review of tetanus in individuals with previous tetanus toxoid immunization
J P Hopkins, C Riddle, M Hollidge, S E Wilson
PMID: 29769864 PMCID: PMC5864474 DOI: 10.14745/ccdr.v40i17a03 https://pubmed.ncbi.nlm.nih.gov/29769864/
"Tetanus spores are ubiquitous and this report clearly documents that tetanus cases can occur in individuals previously immunized with tetanus toxoid vaccine. Clinicians should not rule out tetanus when clinical symptoms suggest it, regardless of the vaccination history. "Immunisation does not rule out tetanus; David R Vinson, staff physician
BMJ. 2000 Feb 5; 320(7231): 383. PMCID: PMC1127160 PMID: 10657350
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1127160/
"A number of rare and exceptional cases of tetanus occur despite adequate immunisation and protective levels of neutralising antibodies. Since tetanus is likely to be fatal if not recognised and treated properly, the caveat from Shimoni et al1 merits repeating: doctors should entertain the diagnosis of tetanus in the proper clinical setting, regardless of the patient's immunisation record. "
Immunization does not interfere with uptake and transport by motor neurons of the binding fragmentof tetanus toxin
Paul S Fishman, Christopher C Matthews, Deborah A Parks, Michael Box, Neil F Fairweather
PMID: 16557581 DOI: 10.1002/jnr.20847
Tetanus in an immunised patient Zvi Shimoni, Anatoly Dobrousin, Jonathan Cohen, Silvio Pitlik
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1116846/
"We report a case of severe generalised tetanus in a patient who had been immunised fully."
Severe tetanus in immunized patients with high anti-tetanus titers N E Crone, A T Reder https://pubmed.ncbi.nlm.nih.gov/1565228/
""Severe (grade III) tetanus occurred in three immunized patients who had high serum levels of anti-tetanus antibody. The disease was fatal in one patient. One patient had been hyperimmunized to produce commercial tetanus immune globulin.""The diagnosis of tetanus, nevertheless, should not be discarded solely on the basis of seemingly protective anti-tetanus titers."
Localized Tetanus in an Adult Patient: Case Report. Gulamhussein MA, Li Y, Guha A.J Orthop Case Rep. 2016 Sep-Oct;6(4):100-102. doi: 10.13107/jocr.2250-0685.592.PMID: 28164065 Free PMC article.
"Of all the cases described in literature, generalized tetanus is by far the most common presentation, but it may also present as neonatal tetanus, cephalic tetanus, and localized tetanus, the latter two being much rarer. In this case report, we present the rare form i.e., localized tetanus in an adult male with a history of minimal trauma as well as a late, unusual mode of presentation."
https://pubmed.ncbi.nlm.nih.gov/28164065/
Localized tetanus mimics acute perforated viscus: A diagnostic challenge and review of case reports.
Idris I, Mafauzy MM, Baharuddin KA, Alwi F, Mohamad WSW.Turk J Emerg Med. 2022 Sep 30;22(4):226-229. doi: 10.4103/tjem.tje https://pubmed.ncbi.nlm.nih.gov/36353387/
Progressive localized tetanus in patient with inadequate human tetanus immunoglobulin therapy
Daniel Licindo,a,⁎ Evan Matthew Putra,b Medianto Rombetasik,c and Heriyanto Limd
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8122171/
Truncal tetanus: a case report. Bağcı Z.J Trop Pediatr. 2021 Jan 29;67(1):fmaa129. doi: 10.1093/tropej/fmaa129.PMID: 33411936
"Localized tetanus is a rare form of tetanus that can progress to generalized tetanus. CASE: In this report, we present a case of localized tetanus in a 9-year-old boy who had never been vaccinated against tetanus. ..."
https://pubmed.ncbi.nlm.nih.gov/33411936/
Localized tetanus in immunized mice.
Fishman PS, Parks DA, Bowen T, Matthews CC.Neurotoxicology. 2009 Jul;30(4):697-701. doi: 10.1016/j.neuro.2009.05.004. Epub 2009 May 22.PMID: 19465055
"Although vaccination dramatically increases resistance to tetanus toxin, by virtue of its extremely high potency, the toxin can produce prolonged localized tetanus even in vaccinated animals with relatively small amounts of protein. ..."
Presumed localized tetanus in two cats.
Polizopoulou ZS, Kazakos G, Georgiadis G, Soubasis N, Koutinas Ch, Koutinas AF.J Feline Med Surg. 2002 Dec;4(4):209-12. doi: 10.1053/jfms.2001.0184.PMID: 12468315
[Localized tetanus in Abidjan: clinical and prognostic features (1976-1997)].
Kakou AR, Eholie S, Ehui E, Ble O, Bissagnene E, Aoussi E, Odehouri K, Kadio A.Bull Soc Pathol Exot. 2001 Nov;94(4):308-11.PMID: 11845522 French.
A Rare Case of Localized Tetanus.
Sharma DS, Shah MB.Indian J Crit Care Med. 2018 Sep;22(9):678-679. doi: 10.4103/ijccm.IJCCM_182_18.PMID: 30294137
Presentations of tetanus include generalized tetanus, neonatal tetanus, cephalic tetanus, and localized tetanus, the latter two being much rarer. We present case of a 55-year-old male farmer, presented with an injury to the left toe. ...
https://pubmed.ncbi.nlm.nih.gov/30294137/
[Chronic localized tetanus in a patient presenting chronic post-traumatic ulcerations of the legs].
THIERS H, COLOMB D, FAYOLLE J, MOULIN G, TAINE B.Lyon Med. 1957 Jul 7;89(27):14-5.PMID: 13464155 French. No abstract available. https://pubmed.ncbi.nlm.nih.gov/13464155/
Acquiring Tetanus After Hemorrhoid Banding and Other Gastrointestinal Procedures
John Afshin Kasher![]() 1,3 and Glenn Mathisen2 J Gastrointest Surg. 2007 Apr; 11(4): 515–519. Published online 2007 Jan 17. doi: 10.1007/s11605-006-0079-6 PMCID: PMC1852382 PMID: 17436138
1,3 and Glenn Mathisen2 J Gastrointest Surg. 2007 Apr; 11(4): 515–519. Published online 2007 Jan 17. doi: 10.1007/s11605-006-0079-6 PMCID: PMC1852382 PMID: 17436138
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1852382
Localised Tetanus: Rare Presentation Of A ‘Forgotten’ Disease Dr Vineeta Gupta, Dr Shashikant Dewangan, Prof Bal Dev Bhatia First published: 15 March 2011 https://doi.org/10.1111/j.1440-1754.2011.02007.
Recurrent generalized tetanus: a case report.
Alhaji MA, Mustapha MG, Ashir GM, Akuhwa RT, Bello MA, Farouk AG.Trop Doct. 2011 Apr;41(2):127-8. doi: 10.1258/td.2010.100338.PMID: 21421889
We describe recurrent generalized tetanus in a four-year-old unimmunized boy following recurrent suppurative otitis media (SOM) within an 11-month period. There are not many published reports on recurrent tetanus. We highlight the importance of both primary immuniza …
Tetanus secondary to oral and odontogenic infections: a case report and systematic literature review Edinson Dante Meregildo-Rodriguez,corresponding author1 Martha Genara Asmat-Rubio,2 and Gustavo Adolfo Vásquez-Tirado2 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9994836/
"Since the diagnosis of tetanus is merely clinical, it is crucial to have a high index of suspicion to diagnose this disease correctly. Although odontogenic tetanus is rare, it is potentially life-threatening."
Lindley-Jones M, Lewis D, Southgate JL.Lancet. 2004 Jun 19;363(9426):2048. doi: 10.1016/S0140-6736(04)16455-6.PMID: 15207956 No abstract available.
[Recurrent tetanus and recrudescent tetanus].
Tavares W, Keim LS, Torres Filho SR, de Oliveira SA, Dias M.Rev Inst Med Trop Sao Paulo. 1982 Mar-Apr;24(2):107-15.PMID: 6127779 Portuguese. No abstract available.
Praharaj KC.J Indian Med Assoc. 1972 Jan 1;58(1):11-2.PMID: 5021266 No abstract available.
Spenney JG, Lamb RN, Cobbs CG.South Med J. 1971 Jul;64(7):859 passim. doi: 10.1097/00007611-197107000-00017.PMID: 5090185 No abstract available.
Louzada JL, Louzada GZ.Hospital (Rio J). 1970 Oct;78(4):1109-14.PMID: 5313676 Portuguese. No abstract available.
Montgomery RD.Br Med J. 1968 Jun 29;2(5608):829. doi: 10.1136/bmj.2.5608.829-c.PMID: 5658923 Free PMC article. No abstract available.
Sahadevan MG.Br Med J. 1968 May 25;2(5603):492-3. doi: 10.1136/bmj.2.5603.492-c.PMID: 5648310 Free PMC article. No abstract available.
Wickramasinghe SY, Fernando M.Br Med J. 1967 Dec 2;4(5578):530. doi: 10.1136/bmj.4.5578.530.PMID: 6065991 Free PMC article. No abstract available.
[Recurrent tetanus. Clinical, immunological and therapeutic considerations].
Warter J, Mantz JM, Tempe JD, Otteni JC.Presse Med (1893). 1967 May 20;75(24):1223-6.PMID: 6024174 French. No abstract available.
VAKIL BJ, MEHTA AJ, TULPULE TH.Postgrad Med J. 1964 Oct;40(468):601-3. doi: 10.1136/pgmj.40.468.601.PMID: 14220407 Free PMC article. No abstract available.
12
[RECURRENT TETANUS (REPORT OF 2 CASES)].
HUANG I, YU CC.Zhonghua Wai Ke Za Zhi. 1963 Dec;11:961.PMID: 14124577 Chinese. No abstract available.
13
CAIN HD, FALCO FG.Calif Med. 1962 Jul;97(1):31-3.PMID: 13875596 Free PMC article. No abstract available.
14
Recurrent tetanus: report of a case.
ALHADY SM.Med J Aust. 1961 Aug 5;48(2):219-20. doi: 10.5694/j.1326-5377.1961.tb69428.x.PMID: 13682404 No abstract available.
15
[Contribution to the problem of recurrent tetanus].
ALZHEIMER O, BROSER F.Nervenarzt. 1961 Jul;32:324-6.PMID: 13682854 German. No abstract available.
16
LUCAS AO.West Afr Med J. 1961 Apr;10:101-3.PMID: 13763955 No abstract available.
17
Recurrent tetanus: report of a case.
MARTIN HL, McDOWELL F.Ann Intern Med. 1954 Jul;41(1):159-63. doi: 10.7326/0003-4819-41-1-159.PMID: 13171801 No abstract available.
18
[A case of delayed, recurrent tetanus].
DE FEO V.Osp Maggiore. 1952 Feb;40(2):72-5.PMID: 14948247 Undetermined Language. No abstract available.
19
[Atypical and recurrent tetanus].
MOBUS L.Z Kinderheilkd. 1950;68(5):427-36.PMID: 14789085 Undetermined Language. No abstract available.
An unusual case of chronic relapsing tetanus associated with mandibular osteomyelitis.
Wakasaya Y, Watanabe M, Tomiyama M, Suzuki C, Jackson M, Fujimuro M, Kimura T, Seino Y, Kawarabayashi T, Yamamoto-Watanabe Y, Matsubara E, Shirahama I, Takamura A, Nakahata N, Shoji M.Intern Med. 2009;48(15):1311-3. doi: 10.2169/internalmedicine.48.2136. Epub 2009 Aug 3.PMID: 19652437 Free article.
However in spite of injections of tetanus toxoid, symptoms of tetanus returned when the administration of metronidazole was discontinued because the infectious focus could not be completely removed. This is the first report of chronic relapsing tetanus associated wi …
2
Bates I.Trop Doct. 1988 Oct;18(4):192.PMID: 3194955 No abstract available.
3
Relapsing tetanus (a case report).
Bhatt AD, Dastur FD.J Postgrad Med. 1981 Jul;27(3):184-6.PMID: 7299709 Free article. No abstract available.
4
[Relapsing tetanus (author's transl)].
Stöhr M, Nerke O.MMW Munch Med Wochenschr. 1976 Jan 9;118(2):35-8.PMID: 814422 German.
Obstetric tetanus in an immunized patient.
Principe-Collazos J, Ramos-Yataco A, Uribe AGG, Cahuayme-Zuniga L, Arevalo I, Delgado-Cáceres FM.IDCases. 2022 Jul 12;29:e01568. doi: 10.1016/j.idcr.2022.e01568. eCollection 2022.PMID: 35855941 Free PMC article.
Obstetric tetanus is defined as a C. tetani infection that occurs during pregnancy or within six weeks of delivery. In Peru, there are no reports of obstetric tetanus cases. Here we report a sixth case of obstetric tetanus in a puerperal woman who underwent c …
2
Cephalic tetanus manifesting as isolated facial nerve palsy- a case report from rural Armenia.
Kishmiryan A, Gautam J, Acharya D, Singh BM, Ohanyan A, Arakelyan A, Vahanyan A, Shoura S.J Infect Dev Ctries. 2021 Nov 30;15(11):1770-1773. doi: 10.3855/jidc.13817.PMID: 34898510 Free article.
Cephalic tetanus is a rare clinical form of tetanus, clinically characterized by trismus and cranial nerve palsy involving one or more cranial nerves, facial nerve being the most common. We report a case of cephalic tetanus with left-sided lower motor facial …
[Tetanus after cat scratch and bites in a previously immunized patient].
Fica A, Gaínza D, Ortigosa P.Rev Chilena Infectol. 2017 Apr;34(2):181-185. doi: 10.4067/S0716-10182017000200012.PMID: 28632833 Free article. Spanish.
Tetanus is declining due to vaccination, professional labor management and appropriate wound care. Tetanus cases have been reported despite immunization. We report the case of a previously healthy 21 years old female patient that presented a mild generalized teta …
Tetanus: the 'forgotten disease'. A rare cause of dysphagia and trismus.
Tahery J, Morris DP, Birzgalis AR.J Laryngol Otol. 2004 Dec;118(12):974-6. doi: 10.1258/0022215042790529.PMID: 15667686
Tetanus kills approximately 500 000 people worldwide each year. Widespread immunization has ensured that it is rarely encountered in the United Kingdom. An increase in global travel may increase the likelihood of such encounters in the developed world in the future. In the …
Emerg Infect Dis. 2014 Sep; 20(9): 1571–1573.
PMCID: PMC4178411
PMID: 25152389
Clostridium tetani Osteitis without Tetanus
Pierre-Yves Levy, Pierre-Edouard Fournier, Laurène Lotte, Matthieu Million, Philippe Brouqui, and Didier Raoult![]()
[Localized tetanus after esophagogastrectomy].
Becq-Giraudon B, Barbier J, Meriel P, Garnier D, Montaz N, Carretier M.J Chir (Paris). 1983 Oct;120(10):543-5.PMID: 6655000 French.
23
[Unusual course of localized tetanus].
Kostrzewski JM.Przegl Epidemiol. 1983;37(3-4):463-5.PMID: 6665206 Polish. No abstract available.
24
Tetanus: review of the literature and report of a case.
Smith MJ, Myall RW.Oral Surg Oral Med Oral Pathol. 1976 Apr;41(4):451-6. doi: 10.1016/0030-4220(76)90272-3.PMID: 772513
The clinical features, active and passive immunization schedules, and an approach to management of established tetanus are reviewed and discussed. A case of localized tetanus is presented in which the patient's initial complaint was inability to open the mouth. ...
25
[Localized tetanus (apropos of 19 cases studied in Dakar)].
Diop Mar I, Durieux P, Badiane S.Bull Soc Med Afr Noire Lang Fr. 1974;19(4):392-6.PMID: 4465054 French. No abstract available.
26
Tetanus toxin in dissociated spinal cord cultures: long-term characterization of form and action
W H Habig, H Bigalke, G K Bergey, E A Neale, M C Hardegree, P G Nelson
PMID: 3734804
DOI: 10.1111/j.1471-4159.1986.tb00700.x